

John Murphy, MDLinx | August 29, 2018
Medical marijuana is now legal in 30 states and the District of Columbia. If it’s been legalized in your state, or it looks like it might be legalized soon, you probably want to know how to answer if a patient asks you about it. First, it’s not as easy or as straightforward as writing a prescription for, say, an antibiotic. Several steps are involved, and the regulations are different in each state.

Physicians can’t ‘prescribe’ medical marijuana, but they can recommend it for certain patients. In some states, physicians must be registered to make a recommendation.
Henry S. Levine, MD, spoke with MDLinx to explain some of the ground rules for “prescribing” medical marijuana. Dr. Levine is a board-certified psychiatrist with a specialty in forensic psychiatry in Bellingham, WA, and lectures widely on psychopharmacology and the uses and hazards of medical marijuana.
How do you prescribe medical marijuana?
First of all, you can’t actually “prescribe” it—you can “authorize” or “recommend” that a patient obtain it.
“The core of this problem lies in the Federal Government’s stance that marijuana is an illegal substance in all cases and has ‘no currently accepted medical use (Controlled Substances Act, 1970),’” Dr. Levine said. Cannabis is a Schedule I controlled substance and, under the Controlled Substances Act, physicians cannot legally prescribe a Schedule I controlled substance.
However, a federal court decision found that while a prescription for cannabis is unlawful, a recommendation is allowed. A recommendation is not considered an order, but a communication between doctor and patient on benefits and harms. As such, states can step in to establish protections for patients who receive recommendations, along with a regulatory framework for the production and distribution of cannabis.
Some states require physicians to be registered; other states, such as Dr. Levine’s state of Washington, allow any physician to recommend medical marijuana use. (Incidentally, many states permit not only MDs and DOs to recommend medical marijuana, but also physician assistants, certain nurse practitioners, and other healthcare personnel. We’ll simply use “physician” for this article.)
How do you become registered?
“These laws and regulations differ dramatically, not just in the terms used, but from state to state,” Dr. Levine said. Some states, such as New York, require physicians to be in good standing, be qualified to treat patients with certain serious conditions, and take a 2- to 4-hour continuing education course on medical marijuana before they can provide patients with recommendations (called “certifications” in New York).
Although the scientific evidence for marijuana’s safety and efficacy in treating specific conditions is still lacking, there are any number of conditions for which states authorize its use, Dr. Levine noted. “California’s 1996 law allows a physician to permit use of medical marijuana ‘for treatment of cancer, anorexia, AIDS, chronic pain, spasticity, glaucoma, arthritis, migraine, or any other illness for which marijuana provides relief’—most physicians read that as ‘anything goes.’ Washington specifies a list of only 9 conditions, Illinois 44,” he said.
“In all cases, I strongly recommend that potential endorsers know their own state laws and requirements,” he added. Sources for this information can be found at the National Conference of State Legislatures website and at ProCon.org.
Once registered, what do you do when a patient asks for a medical marijuana recommendation?
You don’t just write the recommendation and send the patient on his or her way. “An important thing for a physician to do to avoid being labeled a ‘marijuana mill’ is to establish that a true doctor-patient relationship has been formed,” Dr. Levine explained.
This means that physicians should perform and record an adequate history, including of the condition potentially being treated by medical marijuana, and any conditions that may present contraindications to medical marijuana use, such as liver disease, psychiatric disorders, and addiction. The history should also include: past and current treatment history; addiction history, including family history; the patient’s psychosocial circumstances and supports; and pregnancy, menstrual, and contraception data if the patient is female.
“The physician should ensure the performance of an adequate physical examination or should perform one themselves,” Dr. Levine added. “They may educate the patient about alternative treatments and risks associated with medical marijuana use, and safety precautions regarding the supply of medical marijuana to protect others, such as children and pets, who may have access to their supply. They may educate the patient about the pros and cons of the various routes of administration available for medical marijuana. Last but not least, they should in all cases in which medical marijuana is permitted formulate a treatment and follow-up plan.”
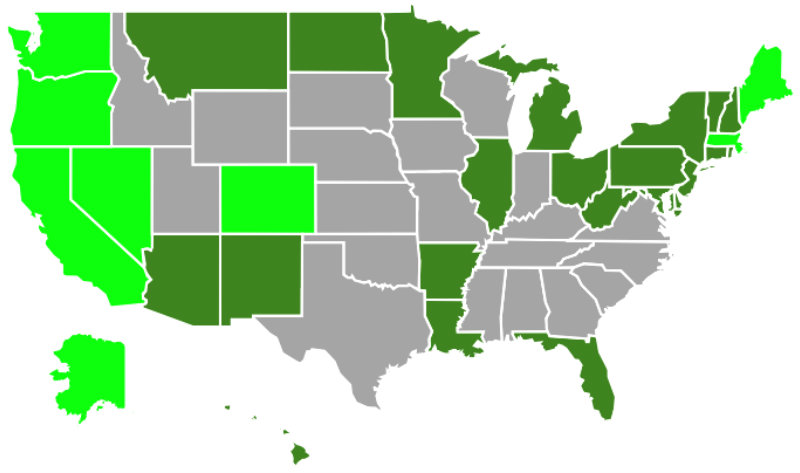 Medical marijuana is now legal in 30 states and the District of Columbia (states in light green and dark green; states in gray have not legalized marijuana for medical or recreational use).
Medical marijuana is now legal in 30 states and the District of Columbia (states in light green and dark green; states in gray have not legalized marijuana for medical or recreational use).
All of this must be documented. (This helpful cannabis medical checklist for health-care practitioners is available for download from a Canadian nonprofit.) Documentation of follow-up visits might include recording progress toward treatment goals, use of quantitative urinary/blood drug screening and monitoring, validated quality of life measurements, and a written patient contract.
“The contract might include a provision for the patient to provide a copy of each receipt for purchase of medical marijuana,” Dr. Levine explained. “Documentation should as well include a strategy for dosing, which should reflect the philosophy of starting low, going slow, staying low, using as little as possible to achieve benefit and avoid undesirable effects. Many physicians have the patient keep a log of each use and a dosing journal that the physician copies and keeps in the patient chart.”
What does the recommendation look like? Is it like a written prescription?
“A medical marijuana recommendation is written on a different form, specifically not on a prescription form, and cannot be filled at a pharmacy,” Dr. Levine said. (Click here for an example of a recommendation.)
“Depending on the state, it is taken to a dispensary, commercial shop, or state-approved facility where a patient can purchase a variety of quantities of medical marijuana of differing chemical makeup for varying lengths of time,” he explained. “The product they receive may or may not be regulated and inspected for its chemical contents and purity. The product’s labeling may or may not tell the patient much about what they are receiving, or how to use it to best advantage. This is almost always left up to the patient to determine.”
Unlike a registered pharmacist, the person behind the counter at the dispensary may or may not be trained in educating the patient about the medical marijuana product, which is paid entirely out of pocket by the patient and is not covered by insurance.
After making the recommendation, what’s the physician’s obligation to the patient?
“Speaking as a forensic psychiatrist, I have seen no published US standards that can answer this question,” Dr. Levine said. “Therefore, I think it safest for physicians to assume that they have the same obligations for care as they would if they were prescribing a scheduled controlled substance.”
Bottom line—what are the pros and cons of recommending medical marijuana?
“The most potent ‘pro’ in endorsing medical marijuana is that it allows access to another ‘arrow in the quiver’ of physicians in helping patients, particularly those persons fighting pain, certain neurological conditions, and possibly other medical conditions as well, including some psychiatric disorders,” Dr. Levine said.
“The most potent ‘con’ is that it is an addictive substance, particularly during adolescence, that can also increase the risks of developing psychosis, and can cause falls, driving accidents, cognitive losses, cardiopulmonary complications, and reproductive dangers, including very negative effects on the developing fetus, as well other potential adverse effects,” he noted.
“It is my impression, having spoken with many colleagues about this issue, that most physicians make the decision on whether to endorse medical marijuana based on their emotional opinions on marijuana’s effects, rather than on a scientific understanding of its known effects, helpful and adverse. This is unfortunate,” Dr. Levine said.
Although there’s much we don’t know about its effects, he added, we do know enough about marijuana science to make rational, data-based decisions in practice.
Therefore, “it is vitally important that more physicians avail themselves of courses on medical marijuana given by the various specialty organizations and other entities, as well as the online courses available through most health departments in states that allow medical marijuana endorsements.” (See materials available from the state of Washington, for example.)
“It is my hope that physicians will increasingly make the pro vs con decision on endorsing medical marijuana based on science and knowledge, rather than emotion,” Dr. Levine concluded.


